
In vitro fertilization
In Vitro Fertilization
Have you ever wondered how In vitro fertilization works?
Or which options do I have, if natural conception does not work for me?
What is in vitro fertilization?
In vitro fertilization (IVF) is a sophisticated set of techniques used to help with fertility, avoid genetic issues, and aid in child conception. An “In vitro” procedure means that it has been performed or is taking place in a test tube, culture dish, or elsewhere outside a living organism. So it means that the fertilization is done outside the woman’s body in a laboratory.
IVF is the type of assisted reproduction technique that works the best, however, it is not the only one. Besides IVF we also have:
- artificial insemination
- intrauterine insemination (IUI)
- Gamete intrafallopian transfer (GIFT)
- Pronuclear stage tubal transfer (PROST)
- Tubal embryo transfer (TET)
- Zygote intrafallopian transfer (ZIFT).
Who is suitable for In vitro fertilization?
In vitro fertilization (IVF) is a treatment for infertility or genetic problems. Usually, IVF is not the first option for most couples that cannot get pregnant naturally since they may be able to try less invasive treatment options before attempting IVF, such as fertility medications to boost egg production or IUI, in which sperm are placed directly in the uterus close to the time of ovulation.
IVF is occasionally recommended as the first line of therapy for infertility in women over the age of 40. If you have specific medical issues, IVF may still be an option. IVF, for instance, could be a choice if you or your partner have:
- Fallopian tube damage or blockage. Fallopian tube damage or blockage makes it difficult for an egg to be fertilized or for an embryo to travel to the uterus.
- Ovulation disorders. If ovulation is infrequent or absent, fewer eggs are available for fertilization.
- Endometriosis. Endometriosis occurs when tissue similar to the lining of the uterus implants and grows outside of the uterus — often affecting the function of the ovaries, uterus and fallopian tubes.
- Uterine fibroids. Fibroids are benign tumors in the uterus. They are common in women in their 30s and 40s. Fibroids can interfere with implantation of the fertilized egg.
- Previous tubal sterilization or removal. Tubal ligation is a type of sterilization in which the fallopian tubes are cut or blocked to permanently prevent pregnancy. If you wish to conceive after tubal ligation, IVF may be an alternative to tubal ligation reversal surgery.
- Impaired sperm production or function. Below-average sperm concentration, weak movement of sperm (poor mobility), or abnormalities in sperm size and shape can make it difficult for sperm to fertilize an egg. If semen abnormalities are found, a visit to an infertility specialist might be needed to see if there are correctable problems or underlying health concerns.
- Unexplained infertility. Unexplained infertility means no cause of infertility has been found despite evaluation for common causes.
- A genetic disorder. If you or your partner is at risk of passing on a genetic disorder to your child, you may be candidates for preimplantation genetic testing — a procedure that involves IVF. After the eggs are harvested and fertilized, they’re screened for certain genetic problems, although not all genetic problems can be found. Embryos that don’t contain identified problems can be transferred to the uterus.
- Fertility preservation for cancer or other health conditions. If you’re about to start cancer treatment — such as radiation or chemotherapy — that could harm your fertility, IVF for fertility preservation may be an option. Women can have eggs harvested from their ovaries and frozen in an unfertilized state for later use. Or the eggs can be fertilized and frozen as embryos for future use.
- A lesbian couple that wants to do the ROPA method where the egg of one of the women is fertilized with a donor sperm and implanted in the other woman.
- Although its ethics are into debate, women who don’t have a functional uterus or for whom pregnancy poses a serious health risk might choose IVF using another person to carry the pregnancy (gestational carrier). In this case, the woman’s eggs are fertilized with sperm, but the resulting embryos are placed in the gestational carrier’s uterus.
- A single woman that wants to get pregnant but has failed to do so via artificial insemination or, wants to select the embryo due to a genetic disorder.
How does In vitro fertilization work?
IVF cycles typically last two to three weeks and it can take more than one cycle. Each cycle has some steps being ovarian stimulation, egg retrieval, sperm retrieval, fertilization, and embryo transfer milestones in the IVF process.
1. Ovulation induction
Instead of the solitary egg that ordinarily develops each month, the ovaries are stimulated to generate numerous eggs at the beginning of an IVF cycle using synthetic hormones. You may be wondering why, if you only want one baby, that many eggs are needed. Well, it is basically because some eggs won’t fertilize or develop normally after fertilization and having more than one option is better since it increases the probabilities of success.
In order to achieve the desired number of eggs, different drugs are used, including:
- Medications that stimulate the ovaries. You can be given an injectable medicine that contains follicle-stimulating hormone (FSH), luteinizing hormone (LH), or a combination of both to activate your ovaries. These drugs encourage the simultaneous development of several eggs as learned in the ovogenesis post.
- Oocyte maturation medications. You will be prescribed human chorionic gonadotropin (HCG) or other drugs to help the eggs develop when the follicles are prepared for egg retrieval, which typically occurs after eight to 14 days.This is the hormone that is detected in a pregnancy test.
- Prescription drugs to stop early ovulation. These drugs stop your body from prematurely releasing the eggs in development to ensure that any egg is lost.
- Medications that will get your uterus ready. Your doctor may advise that you start taking progesterone supplements the day of egg retrieval or at the day of embryo transfer to help the lining of the uterus thicken.
Before your eggs are prepared for retrieval, you usually need to undergo ovarian stimulation for one to two weeks. When the eggs are ready to be picked up, you may have:
- Vaginal ultrasound is an imaging test of your ovaries that tracks the growth of follicles, the fluid-filled sacs in your ovaries where eggs develop.
- Blood tests are used to assess how well you are responding to ovarian stimulation drugs. Typically, estrogen levels rise as follicles form and progesterone levels fall until after ovulation.
At this point two things can happen. Luckily everything will be alright and the IVF process will continue as planned. However, sometimes and for one of the following reasons, IVF cycles may need to be stopped before egg retrieval: insufficient follicle development, untimely ovulation,too many follicles developing increasing the risk of ovarian hyperstimulation syndrome or other medical issues.
If it’s the case that the process must be stopped, the doctor may advise you to get an egg donor. Nonetheless, sometimes it is just a matter of redistributing the drugs and the doses and trying again.
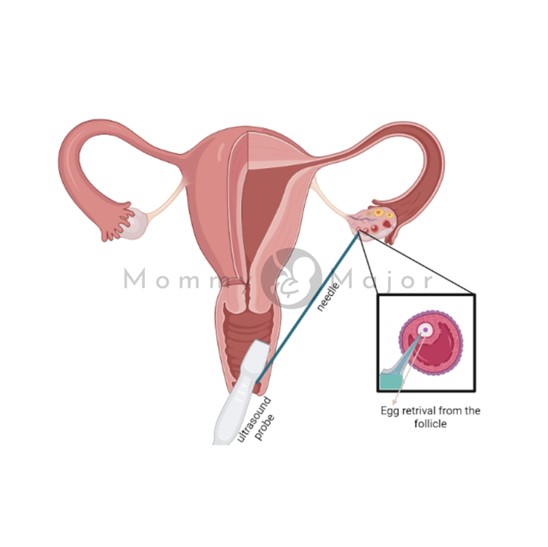
2. Egg retrieval
The egg retrieval process is usually done in a clinic or in your doctor’s office. YThis procedure is done 34 or 36 hours after the last injection and prior to ovulation. You’ll be sedated and given painkillers for egg retrieval since it is a simple surgical intervention.
The most common type of retrieval is transvaginal ultrasound aspiration. Your vagina is probed with an ultrasound device to find follicles. Besides, an abdominal ultrasound could be utilized to guide the needle if transvaginal ultrasound can’t reach your ovaries.
The eggs are then extracted by passing a small needle needle attached to a suction tool into the vagina and into the follicles using ultrasound guidance. Many eggs can be extracted in around 20 minutes.
Mature eggs are placed in a nutritive liquid (culture medium) and incubated. Eggs that appear healthy and mature will be mixed with sperm to attempt to create embryos.
After egg retrieval, you may experience cramping and feelings of fullness or pressure.
3. Sperm retrieval
A semen sample must be given at your doctor’s office or clinic the morning of egg retrieval either if you’re utilizing your partner’s sperm or a donor’s sperm. Usually, masturbation is used to get the semen sample. It is occasionally necessary to utilize additional techniques, such as testicular aspiration, which involves using a needle or surgical procedure to remove sperm straight from the testicle.
In a laboratory, semen fluid and sperm are separated in order to facilitate later on the fertilization process.
4. Fertilization
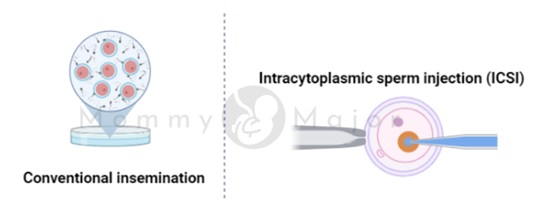
The clinic can try fertilization using two popular techniques:
- Conventional insemination. Healthy sperm and mature eggs are combined during traditional insemination, and they are then incubated overnight. This technique is used when the reason why the treatment is performed does not involve defects in either sperm or eggs.
- Intracytoplasmic sperm injection (ICSI). Each mature egg is directly injected with one healthy sperm during ICSI. When semen quantity or quality (for example, the sperm is unable to swim) is an issue, or if fertilization attempts during previous IVF cycles were unsuccessful, ICSI is frequently performed.
5. Extra procedures
Before embryo transfer, your doctor might advise extra procedures in some circumstances.
- Assisted hatching. An embryo “hatches” from its surrounding membrane (pellucid zone) about five to six days after fertilization as we can learn in the fertilization post. This enables it to implant into the lining of the uterus. Your doctor could advise assisted hatching, a procedure in which a hole is cut in the zona pellucida shortly before transfer to aid the embryo in hatching and implantation, if you’re an older woman or if you’ve had numerous unsuccessful IVF efforts.
The procedure of assisted hatching can stiffen the zona pellucida, which is beneficial for eggs or embryos that have previously been frozen.
- Genetic testing before implantation. Embryos are left to develop in the incubator for around five to six days, or until a small sample can be taken and examined for certain genetic disorders or the right number of chromosomes. This procedure is advised when the cause of a genetic disorder is known in order to avoid having children with the disease.
6. Embryo transfer
Embryo transfer typically happens two to five days after the egg retrieval and is performed in a clinic or at your doctor’s office. A moderate sedative may be administered, although the operation is mostly painless, you can feel a little cramping.
The medical professional will place a catheter—a long, thin, flexible tube—into your vagina, through your cervix, and into your uterus. The catheter’s tip is connected to a syringe that holds one or more embryos suspended in a little volume of fluid allowing the doctor to inject the embryo or embryos into your uterus.
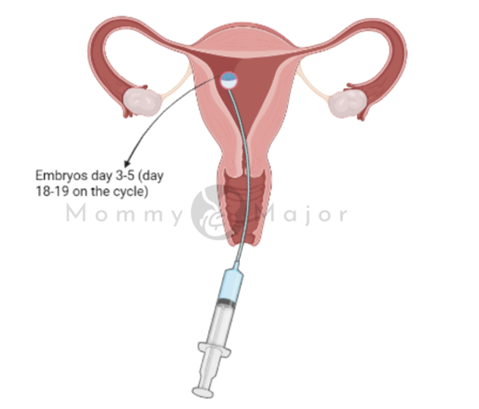
If successful, an embryo will implant in the lining of your uterus about six to 10 days after egg retrieval.
7. After the procedure
Your regular daily activities can be resumed after the embryo transfer. Your ovaries could still be swollen, though, so you should take into account avoiding strenuous activities, which could be uncomfortable.
Side effects
After the procedure some side effects may appear, it is better if you are prepared and informed to avoid scars. Common negative effects include:
- Passing a tiny amount of clear or red fluid soon after the procedure as a result of the cervix being swabbed prior to the embryo transfer.
Breast sensitivity brought on by excessive estrogen levels. - Slight bloating
- Light cramps
- Constipation
- Passing a tiny amount of clear or red fluid soon after the procedure as a result of the cervix being swabbed prior to the embryo transfer.
After the embryo transfer, if you experience any moderate to severe pain, call your doctor. The risk of problems like infection, ovarian torsion, and severe ovarian hyperstimulation syndrome will be assessed by the medical professional. However, most of the time women pass the days after the procedure without any symptoms or complications.
For more information check this Pubmed article.
Results
Your doctor will test a sample of your blood to see if you’re pregnant about 12 to 2 weeks after egg retrieval. Sometimes, women also take a pregnancy test before seeing their doctors but it is not the best thing to do. As learned on the pregnancy test post, pregnancy tests detect hCG levels, and as said before, you are given external hCG to facilitate the implantation so the results from the pregnancy test may not be accurate.
- If you’re expecting, your doctor will recommend that you receive prenatal care from an obstetrician or other pregnancy specialist.
- You’ll stop taking progesterone if you’re not pregnant and probably start getting your period within a week. Besides, your doctor might recommend measures you can take to increase your chances of becoming pregnant through IVF if you’re interested in trying another cycle of in vitro fertilization (IVF).
Which are the changes to giving birth to a healthy baby after IVF?
The Society for Reproductive Technology (SART) states that for women under 35, the percentage of live births via IVF is 55.6%. WHen you are over 35, and even more when you are over 40 as learned in the pregnancy when you are in your 40’s post, it is not only more difficult but also riskier so the percentage of successful births decreases.
The likelihood of having a healthy baby following IVF depends on a number of factors, including:
- Mother’s age. The likelihood of becoming pregnant and giving birth to a healthy child using your own eggs via IVF increases with age. Women over the age of 41 are frequently advised to think about utilizing donor eggs during IVF to improve success rates.
- Embryonic stage. Compared to less-developed embryo transfers, more-developed embryo transfers are linked to greater pregnancy rates (day two or three). Not all embryos, nevertheless, make it through the growth stage.
- Reproductive background. Women who have already given birth have a higher chance of success with IVF than women who have never given birth. Women who have used IVF more than once in the past but were unsuccessful in getting pregnant have lower success percentages.
- Cause of infertility. Your chances of having a successful IVF rise if you have a normal egg production. Compared to women with unexplained infertility, those with severe endometriosis have a lower chance of success with IVF.
- Lifestyle. Smokers frequently have fewer eggs removed during IVF and may miscarry more frequently. Smoking can reduce a woman’s success rate with IVF by 50%. Your chances of becoming pregnant and having a child can be lowered if you are obese. Besides the use of alcohol, recreational drugs, excessive caffeine and certain medications also can be harmful.
Risks of IVF
Even Though iVF is a very safe procedure, there are some risks associated with it.
- Multiple births. If more than one embryo is implanted into your uterus through IVF, your risk of having multiple children rises. Compared to pregnancies with a single fetus, pregnancies with multiple fetuses have a higher risk of early labor and low birth weight.Low birth weight and preterm delivery. According to research, there is a tiny chance that a baby produced via IVF would be premature or have a low birth weight.
- Ovarian hyperstimulation syndrome. When used to promote ovulation, injectable fertility medicines like human chorionic gonadotropin (HCG) can lead to ovarian hyperstimulation syndrome, which makes your ovaries uncomfortable and swollen. The normal duration of symptoms, which include minor stomach pain, bloating, nausea, vomiting, and diarrhea, is one week. However, if you get pregnant, your symptoms can last for a few weeks. Rarely, ovarian hyperstimulation syndrome can become more severe, which can lead to fast weight gain and shortness of breath.
- Miscarriage. When fresh embryos are used for IVF, the rate of miscarriage is similar to that of women who conceive naturally and ranges from 15% to 25%; however, the rate rises with maternal age.
- Problems with the egg retrieval process. Egg collection with an aspirating needle may result in hemorrhage, infection, or harm to the intestine, bladder, or blood vessel. Sedation and general anesthesia include risks as well, if employed.
- Ectopic pregnancy. You can learn more about it in the ectopic pregnancy post.
- Birth defects. No matter how the kid is conceived, the mother’s age is the main risk factor for the development of birth abnormalities. Some studies suggest that abnormalities may be more likely to occur in babies created through IVF, however, it is necessary to conduct more research.
- Stress. Financially, physically, and emotionally taxing. IVF use can be stressful on your spouse and yourself, try to get the support you need to get through the ups and downs of infertility treatment from therapists, family, and friends.
Some people still believe that one of the risks of IVF is a higher probability of developing cancer. Although some early research suggested there might be a connection between some drugs used to promote egg formation and the establishment of a particular type of ovarian tumor, more recent research refutes these claims. Breast, endometrial, cervical, or ovarian cancer risk following IVF does not seem to be considerably higher.
Steps to do prior IVF
Going through an IVF process is not easy, either mentally or physically for the women. First, it has to be assessed that there is no other way for you to conceive a healthy baby. If this is the best option you and your partner will probably require a number of screenings before starting an IVF such as:
- Testing for ovarian reserve. Your doctor may perform blood tests to measure the levels of follicle-stimulating hormone (FSH), estradiol (estrogen), and anti-mullerian hormone during the first few days of your menstrual cycle in order to evaluate the number and quality of your eggs. Results from tests, which are frequently combined with an ultrasound of your ovaries, can aid in predicting how your ovaries will react to fertility drugs.
- Semen examination. Your doctor will perform a semen analysis just before the beginning of an IVF treatment cycle if it wasn’t done as part of your first fertility assessment. In case that you are using a donor, this has been done before.
- Screening for infectious diseases. You and your partner will undergo HIV and other infectious disease screenings.
- Mock transferring embryos. To establish the depth of your uterine cavity and the procedure most likely to properly implant the embryos into your uterus, your doctor may perform a mock embryo transfer.
- Exam of the womb. Before you begin IVF, your doctor will check the uterus’ inner lining. In order to create images of your uterine cavity, an ultrasound and a sonohysterography, in which fluid is injected via the cervix into your uterus, may be used. Or it might involve a hysteroscopy, in which a lighted, thin, flexible telescope (hysteroscope) is introduced into your uterus through your vagina and cervix.
What do I ask my doctor before IVF?
Besides all the test that have to be done to assess if you are optimal for an IVF treatment,, you might take into account crucial issues that should be addressed by the doctor, such as:
- How many embryos are planned for transfer? Usually, the number of eggs recovered and age are used to determine the number of embryos to be transferred. More embryos are often transferred because older women have a reduced rate of implantation, with the exception of those who use donor eggs or embryos that have undergone genetic testing.
In order to avoid higher order multiple pregnancies, such as triplets or more, the majority of doctors adhere to strict rules. The number of transferred embryos is regulated by law in various nations. Before the transfer operation, be sure you and your doctor have an agreement on the number of embryos that will be transplanted.
- What will you do with the extra embryos? Excess embryos can be frozen and kept for several years in anticipation of usage. Although most embryos will, not all will survive the freezing and thawing procedure.
Frozen embryos can reduce the cost and invasiveness of future IVF cycles. Nevertheless, you might be able to give any extra frozen embryos to a research facility or another couple. You could also decide to throw away any extra embryos.
- How would you handle a pregnancy with multiples? IVF can lead to a multiple pregnancy, which has health risks for both you and your unborn children, if more than one embryo is implanted into your uterus. Fetal reduction may be utilized in some situations to assist a mother in giving birth to fewer children with fewer health hazards. Yet, choosing to pursue fetal reduction is a significant choice with moral, psychological, and emotional repercussions.
- Have you thought about the potential drawbacks of using gestational carriers, donated eggs, sperm, or embryos? A trained counselor with expertise in donor issues can help you understand the concerns, such as the legal rights of the donor. You may also need an attorney to file court papers to help you become legal parents of an implanted embryo.



